SVIMS JOURNEY TO NABH
NABH (National Accreditation Board for Hospitals and Healthcare
Providers)
is a part of Quality Council of India and an institutional member of
International Society for Quality in Healthcare (ISQua) which provides
accreditation to hospitals which adhere to quality standards.
SVIMS has been providing quality services on par with National and
International standards since its inception. With the increasing demand
for accreditation and with a motive to further improve the services
provided by the institute, SVIMS started its formal quality journey
towards accreditation in March 2015. The requirements for accreditation
are broadly divided into the managerial and clinical components.
Managerial components looks into infrastructure in terms of the
buildings, manpower, equipment, budget etc for patient safety while the
clinical components include measures in place to ensure quality in
patient care and ensuring patient safety.
NABH accreditation can be taken up in two phases i.e. entry level and
the full accreditation. Both these have requirements divided under 10
Chapters. The entry level has 45 standards and 167 objective elements
while the full accreditation has 100 standards and 651 objective
elements. Aiming at full accreditation ground work was initiated for the
full accreditation with teams identified to work for preparation of
manuals, policies, procedures in line with the 100 standards spread
across 10 chapters. Leaders and team members are identified for the 10
chapters. A thorough gap analysis was done to identify what is available
and what needs to be done in all the areas under each chapter wise.
Monthly goals were identified to close the gaps step by step. Audits
were conducted in each area to identify the areas which needed
improvement. Staff had to be trained and motivated to take up this extra
load of maintaining documentation in spite of their already existing
patient and other academic workload. Regular trainings and motivation
helped in maintaining their zeal. Another important components are the
mandatory regulatory licenses.
Once we reached 75-80% of the requirements, we applied in 2016 for the
entry level certification to assess our preparedness for full
accreditation. After inspection, we received the entry level
certification in Dec 2018. With
the confidence gained, we next applied for the full accreditation in
March 2019. Full accreditation takes place in two phases: pre-assessment
and final assessment. The pre-assessment was successfully completed in
Oct 2020. However, due to the COVID pandemic the final assessment was
delayed and was conducted in March 2021. The major noncompliance was
with regard to the fire NOC.
After submission of fire NOC, SVIMS got full accreditation in January,
2022 for a period 3 years i.e. upto January, 2025.
Now we are under Surveillance of NABH status which is expecting in
August, 2023.
Home
Staging of NABH
·
Initiation of NABH
Entry level accreditation - 2015-2016
·
Entry Level
Accreditation certification - Jan 13, 2019 to Jan
12, 2021
·
Initiation of NABH
Full Accreditation - 2019
·
Accreditation Granted
Date - Jan 06, 2022 to Jan 05,
2025
Home
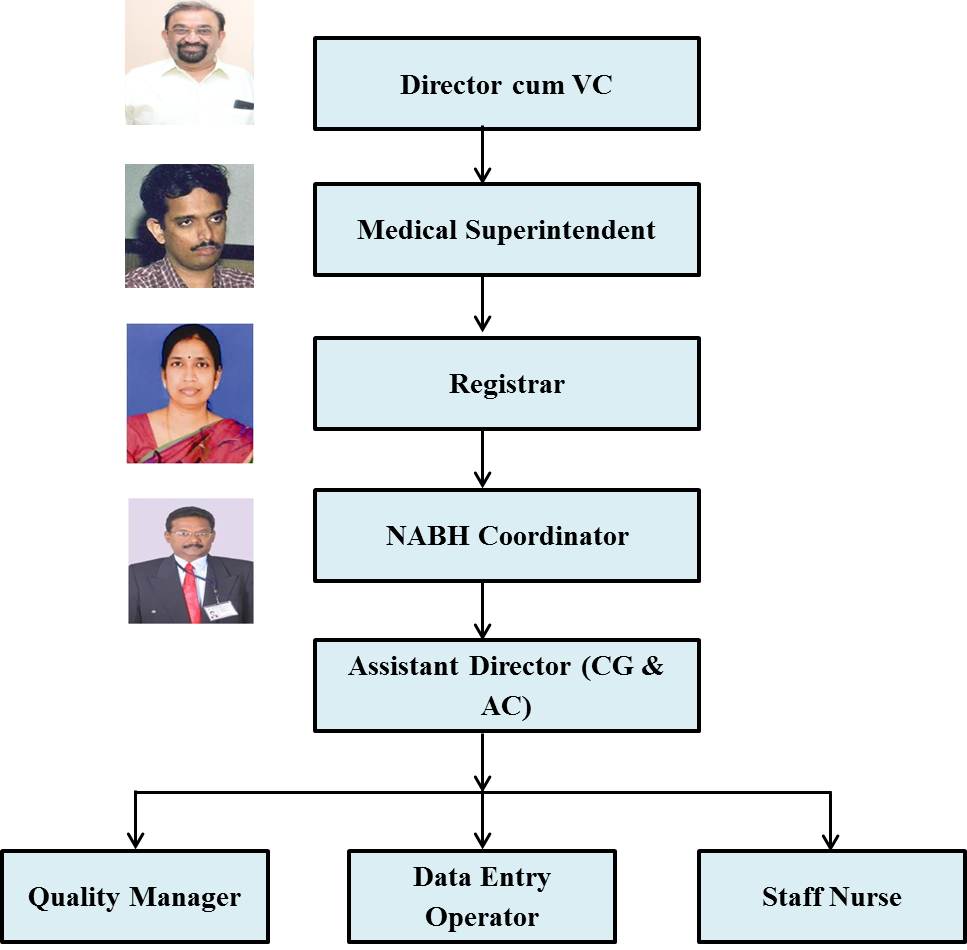
Organogram of SVIMS - CG & AC (NABH)
Home
Ø
Standards of NABH
NABH Consists: -
10 Chapters
-
100 Policies
-
8 Manuals
-
45 SOPs
•
Standards are divided
into 10 chapters, first five chapters are `patient-centric’ and last
five chapters are considered to be `organization-centric’. The standards
are statements that defines the structures and processes that must be
substantially in place in an organization to enhance the quality of
care.
Patient-centric chapters:
•
Access, Assessment and Continuity of Care (AAC)
•
Care of Patients (COP)
•
Management of Medication (MOM)
•
Patient Rights and Education (PRE)
•
Hospital Infection Control (HIC)
Organization-centric chapters:
•
Patient Safety and Quality Improvement (PSQ)
•
Responsibilities of Management (ROM)
•
Facility Management and Safety (FMS)
•
Human Resource Management (HRM)
•
Information Management System (IMS)
Home
Ø
Chapter cum Group Leaders
Chapter: 1 - Access, Assessment and Continuity of Care (AAC)
Group Leader:
Dr. Y. Mutheeswaraiah, Professor & Head, Department of General Surgery
Co
–Ordinator:
Mrs.G. Siresha, Medical Records Officer
|
Task code
(Standard) |
Summary of Standards |
Group Members |
|
AAC 1 |
The organization defines and displays the healthcare services that
it provides |
1.
Mr. V. Rajasekhar, PRO (Lead Member)
2.
Mr. N.V.S. Prasad, MSW
3.
Mr. R. Nagaraja,Sr.Photo Artist |
|
AAC 2 |
The organization has a well-defined registration and admission
process |
1.
Smt.G.Sireesha, MRO (Lead Member)
2.
Sri.K.GiriBabu, AMRO
3.
Smt.N. Hemalatha, H/N, OPD |
|
AAC 3 |
There is an appropriate mechanism for transfer (in and out) or
referral of
patients |
1.
Dr. K. RohithGupta, Asst. Prof., Dept. of EMD (Lead Member)
2.
Dr. P.Subramamyam, Asst. Prof., Dept. of EMD
3.
Mrs. C. Sunitha, NS Gr-I
4.
Smt.C.DhanaRekha, H/N,EMD, |
|
AAC 4 |
Patients cared for by the organization
undergo an established initial assessment |
1.
Dr.A.Sandeep Kumar Reddy, Asst. Prof., Dept. of Medicine(Lead
Member)
2.
Dr.P.Suresh Babu, Deptof General Surgery
3.
Mrs. I. Kanthamma, NS Gr-II |
|
AAC 5 |
Patients cared for by the organization undergo a regular
reassessment |
1.
Dr.A.Sandeep Kumar Reddy, Asst. Prof., Dept. of Medicine (Lead
Member)
2.
Dr.P.SureshBabu, Asst. Prof., Dept. of General Surgery
3.
Mrs.E. Bhuvaneswari NS Gr-II
4.
Smt.N. Hemalatha, H/N, OPD |
|
AAC 6 |
Laboratory services are provided as per the scope of services of the
organization |
1.
Dr. M. M.Suchitra, Professor, Dept. of Biochemistry (Lead Member)
2.
Dr. V. Siva Kumar, Asst. Prof., Dept. of Pathology
3.
Dr.N. Ramakrishna, Asst. Prof., Dept of Microbiology |
|
AAC 7 |
There is an established laboratory quality assurance programme |
1.
Dr. M. M. Suchitra, Professor, Dept. of Biochemistry(Lead Member)
2.
Dr. V. Siva Kumar, Asst. Prof., Dept. of Pathology
3.
Dr. N. Ramakrishna, Asst. Prof., Dept. of Microbiology |
|
AAC 8 |
There is an established laboratory safety programme |
1.
Dr. M. M. Suchitra, Professor, Dept. of Biochemistry (Lead Member)
2.
Dr. V. Siva Kumar, Asst. Prof., Dept. of Pathology
3.
Dr. N. Ramakrishna, Asst. Prof., Dept. of Microbiology
|
|
AAC 9 |
Imaging services are provided as per the scope of services of the
organization |
1.
Dr. S. Sarala, Professor, Dept. of Radiology
(Lead Member)
2.
Mr.S. Balaraju, RSO, Radiotherapy
3.
Dr. R. RamyaPraya, Asst. Prof., Dept. of Nuclear Medicine
4.
Dr.VC. Venkatesh, Lecture, Dept. of Radiology |
|
AAC 10 |
There is an established quality assurance programme for imaging
services |
1.
Dr. S. Sarala, Professor, Dept. of Radiology
(Lead Member)
2.
Dr. R. RamyaPraya, Asst. Prof., Dept. of
Nuclear Medicine
3.
Dr.Harshith Sony, Lecture, Dept. of Radiology |
|
AAC 11 |
There is an established safety programme in the imaging services |
1.
Dr. S. Sarala, Professor, Dept. of Radiology
(Lead Member)
2.
Mr.S. Balaraju, RSO, Radiotherapy
3.
Mr.M.V. Rangarao,Technician Gr.I.
4.
Mr.D. Chandra Sekhar, Tech. Nuclear Medicine |
|
AAC 12 |
Patient care is continuous and multidisciplinary. |
1.
Dr. A. Sandeep Kumar Reddy, Asst. Prof., Dept. of Medicine(Lead
Member)
2.
Mrs. K. Madhavi, Professor & Principal i/c, College of Physiotherapy
3.
Mrs.E. Bhuvaneswari NS Gr.II
4.
Mrs.J. Sarada Devi, NS Gr.II
5.
Mrs. G. Indiramma, NS. Gr.II |
|
AAC 13 |
The organization has an established discharge process. |
1.
Dr. A. LokeswarReddy,Chief MEDCO
(Lead Member)
2.
Dr. K. Vivekanand, CMRO ( Billing)
3.
Mrs. C. Sunitha, NS Gr.I
4.
Mrs.G. Indiramma, NS. Gr.II
5.
Mr. B. Prakash, Security Officer |
|
AAC 14 |
Organization defines the content of the discharge summary. |
1.
Dr. A. Lokeswar Reddy,Chief MEDCO ,
(Lead Member)
2.
Dr. K. Vivekanand, CMRO ( Billing)
3.
Mrs. C. Sunitha, NS Gr.I
4.
Mrs. G.Indiramma, NS. Gr.II |
Chapter: 2 - Care of Patients (COP)
Group Leader:
Dr. Aloka Samantaray, Professor & Head, Dept. of Anesthesiology
Co
–Ordinator:
Dr.Rohit Gupta, Asst. Professor Department of EMD
|
Task code
(Standard) |
Summary of Standards |
Group Members |
|
COP 1 |
Uniform care to patients is provided in all settings of the
organization and is guided by written guidance, and the applicable
laws and regulations |
1.
Dr.V. Chandrasekhar, Asst. Prof.,
Dept. of Community Medicine, (Lead Member)
2.
Dr.A. Lokeswar Reddy, Chief MEDCO |
|
COP 2 |
Emergency services are provided in accordance with written
guidance, applicable laws and regulations. |
Dr. A. Krishna Simha Reddy
Professor, Dept. of Emergency Medicine, |
|
COP 3 |
Ambulance services ensure safe patient transportation with
appropriate care. |
1.
Dr.P. Subramanyam, Asst. Professor
Dept.of EMD, (Lead Member)
2.
Mr. B. Prakash, Security Officer
3.
Mr.Elango Reddy, Fire Safety Officer |
|
COP 4 |
The organization plans and implements mechanisms for the care of
patients during community emergencies, epidemics and other
disasters. |
1.
Dr.P. Subramanyam, Asst.Professor,
Dept.of EMD.
2.
Dr. D.S. Sujith Kumar, Assoc. Professor, Dept. of Community
Medicine. |
|
COP 5 |
Cardio-pulmonary resuscitation services are provided uniformly
across the organization. |
Dr.N.Hemanth, Professor, Dept.of Anaesthesiology |
|
COP 6 |
Nursing care is provided to patients in the organization in
consonance with clinical protocols. |
Dr. M.Nagarathna,Assoc. Professor, College of Nursing, |
|
COP 7 |
Clinical procedures are performed safely |
Dr.P.Hemalatha, Asso. Professor
Dept.of Anaesthesiology |
|
COP 8 |
Transfusion services are provided as per the scope services of the
organization, safely. |
Dr. B.Suresh Babu,Asst. Professor,
Dept.of Transfusion Medicine |
|
COP 9 |
The organization provides care in intensive care and high dependency
units in a systematic manner. |
Dr. V. Sameeraja, Asst.Professor,
Dept.of Medicine, |
|
COP 10 |
Organization provides safe obstetric care. |
Dr.B. Akila, Asst.Professor, Dept.of OBG |
|
COP 11 |
Organization provides safe Pediatric services. |
Dr. P. Puneeth, Assoc. Professor&HoD i/c,Dept.of Paediatrics |
|
COP 12 |
Procedural sedation is provides consistently and safely |
Dr.A.Krishna SimhaReddy,Professor, Dept. of Emergency Medicine |
|
COP 13 |
Anesthesia services are provided in a consistent and safe manner |
Dr. R. Sri Devi, Asst.Professor, Dept.of Anaesthesiology |
|
COP 14 |
Surgical services are provided in a carried out safely. |
1.
Dr. S. B. Amarnath, Assoc. Professor, Dept. of ENT (Lead Member)
2.
Dr. S. Shameem, Asst.Professor,
Dept.of Anaesthesiology |
|
COP 15 |
The organ transplant programme is carried out safely. |
1.
Dr.Ram, Prof & Head,Dept.of Nephrology,
2.
Dr.Ch.Konda Reddy,Dept.of Urology |
|
COP 16 |
The organization identifies and manages patients who are at higher
risk of morbidity/mortality. |
-
Dr.P.JanakiSubhadra, Professor,
-
Dept. of Anaesthesiology
|
|
COP 17 |
Pain management for patients is done in a consistent manner. |
Dr. M. Madhusudan,Assoc. Prof.,Dept. of Anaesthesiology
|
|
COP 18 |
Rehabilitation services are provided to the patients in a safe,
collaborative and consistent manner. |
Mr. K. Senthil Kumar, Asst.Professor,
College of Physiotherapy.
|
|
COP 19 |
Nutritional therapy is provided to patients consistently and
collaboratively. |
Mrs. K. Geetha,Asst. Dietician
|
|
COP 20 |
End of life care is provided in a compassionate and considerate
manner. |
1. Dr.B.V Subramanian, Professor & Head, Dept.of R.T.
2. Dr.D.V.S.Kiran, Asst.Professor,
Dept.of Medical Oncology
|
Chapter: 3 Management of Medication (MOM)
Group Leader
:
Dr. A. UmamaheswarRao, Prof. &HoD, Pharmacology
Co-ordinator:
Dr. K. R. Subash, Professor, Pharmacology & Mr.L.Satheesh, AD Stores
|
Task code
(Standard) |
Summary of Standards |
Group Members |
|
MOM 1 |
Pharmacy services and usage of medication is done safely. |
Dr.K.Vijaya Chandra Reddy, Assoc. Prof, Pharmacololgy |
|
MOM 2 |
The organization develops, updates and implements a hospital
formulary. |
Dr.M.Sravan, Clinical Pharmacist |
|
MOM 3 |
Medications are stored appropriately and are available where
required. |
1.
Mr.L.Satheesh, A.D (Stores)
2.
Dr.Peta.Subramanyam,Sr.Pharmacist |
|
MOM 4 |
Medication are prescribed safely and rationally |
Dr.M.Babu,Asst. Prof, Dept. of Medicine |
|
MOM 5 |
Medication orders are written in a uniform manner. |
Dr.P.Anuhya, Clinical Pharmacist |
|
MOM 6 |
Medication are dispensed in a safe manner. |
1.
Mr.L.Satheesh A.D (Stores)
2.
Dr.Peta.Subramanyam, Sr.Pharmacist
3.
Mrs.T.Prabhavathi, A.D (Nursing) |
|
MOM 7 |
Medication are administered safely. |
1.
Mrs. T. Prabhavathi, A.D (Nursing)
2.
Mrs C. Suneetha, Nursing Suptd., Grade-I
3.
Mrs. E. Bhuvaneswari NS Gr.II
4.
Mrs. J. Sarada Devi, NS Gr.II
5.
Mrs. G. Indiramma, NS. Gr.II
6.
Mrs. I. Kanthamma, NS Gr.II |
|
MOM 8 |
Patients are monitored after medication administration. |
1.
Mrs. T. Prabhavathi, A.D (Nursing)
2.
Mrs C. Suneetha, Nursing Suptd., Grade-I
3.
Mrs. E. Bhuvaneswari NS Gr.II
4.
Mrs. J. Sarada Devi, NS Gr.II
5.
Mrs. G. Indiramma, NS. Gr.II
6.
Mrs. I. Kanthamma, NS Gr-II |
|
MOM 9 |
Narcotic drugs and psychotropic substances, chemotherapeutic agents
and radioactive agents are used safely. |
1.
Dr.T.C.Kalawat, Prof &HoD, Dept. Nuclear Medicine.
2.
Dr.T.Bhargavi, Assoc. Prof, Medical Oncology |
|
MOM 10 |
Implantable prosthesis and medical devices are used in accordance
with laid down criteria. |
Dr. K. Venkat, Assoc. Prof, Dept. of Neurosurgery |
|
MOM 11 |
Medical supplies and consumables are stored appropriately and are
available where required. |
1.
Mr.L.Satheesh, A.D (Stores) &
2.
Dr.Peta.Subramanyam, Sr.Pharmacist |
Chapter: 4 - Patients Rights and Education (PRE)
Group Leaders :
Dr. Rukmangadha, Professor, of Pathology
Co-ordinator :
Mr. NVS. Prasad, MSW
|
Task code
(Standard) |
Summary of Standards |
Group Members |
|
PRE 1 |
The organization protects and promotes patient and family rights and
informs them about their responsibilities during care. |
1.
Dr.Anju Ade, Professor, Dept. Community Medicine,
2.
Mr. K. Giribabu, AMRO
3.
Smt. N. Hemalatha, H/N, OPD |
|
PRE 2 |
Patient and family rights support individual beliefs, values and
involve the
patient and family in decision making processes. |
1.
Dr. N.Sharvani, Asso. Professor, Dept. of Physiology (Lead Member)
2.
Mr. V. Rajasekhar, PRO
3.
Smt. N. Hemalatha, H/N, OPD |
|
PRE 3 |
The patient and/or family members are educated to make informed
decisions and are involved in the care planning and delivery
process. |
1.
Dr. N..Sharvani, Asso. Professor, Dept. of Physiology (Lead Member)
2.
Mrs. P. Sunitha, Head Nurse
3.
Mrs.D. Sailaja, Head Nurse
4.
Mrs. D. Kalavathi, Head Nurse
5.
Mrs. V. Annie Besant, Head Nurse
6.
Mrs. Y. Nirmala, Head Nurse |
|
PRE 4 |
Informed consent is obtained from the patient or family about their
care. |
1.
Dr. K. Venkat, Assoc. Prof, Dept. of Neurosurgery
2.
Mrs.S. Shakira, OT Head Nurse
3.
Mrs. V. Radha Rani, OT Head Nurse
4.
Mr. B. Prasad, Computer Assistant |
|
PRE 5 |
Patient and families have a right to information and education about
their
healthcare needs. |
1.
Dr. K. Prathiba, Assoc. Prof. of Anatomy
2.
Mrs. S. Vahede, Head Nurse,
3.
Mrs. T. Suseela, Head Nurse,
4.
Mrs. T.L. Varalakshmi, Head Nurse,
5.
Mrs. A. Dhanabhagyam, Head Nurse,
6.
Mrs. K. Saraswathi, Head Nurse,
7.
Mrs. A. Premakumari, Head Nurse, |
|
PRE 6 |
Patients and families have a right to information on expected costs. |
1.
Dr. K. Vivekanand, CMRO
2.
Mrs. S. Santhana Lakshmi, Suptd., Credit Cell
3.
Mr. M.L. Govindarajulu, Suptd., Billing Section
4.
Mr. M. Hari, Sr. Asst., Credit Cell |
|
PRE 7 |
The organization has a mechanism to capture patient‘s feedback and
redress of complaints.
|
-
Dr. N. Rukmangadha, Professor &HoD of Pathology,
-
Mr.V. PranayaTeja, Network Engineer,
-
Mr. S. Niranjan, Computer Asst.
-
Mr.N. Dilip, Computer Asst.
|
|
PRE 8 |
The organization has a system for effective communication with
patients
and / or families.
|
1.
Dr. C.V. Praveen Kumar Reddy, Professor, Dept. of Plastic Surgery,
2.
Mrs. E. Bhuvaneswari NS Gr.II
3.
Mrs. J. Sarada Devi, NS Gr.II
4.
Mrs. G. Indiramma, NS. Gr.II
5.
Mrs. I. Kanthamma, NS Gr.II |
Chapter: 5 Hospital Infection Control (HIC)
Group Leader :Dr.
R. Jayaprada, Assoc. Prof. of Microbiology
Co-Ordinator :Dr.
N. Ramkrishna, Asst. Prof. of Microbiology
|
Task code
(Standard) |
Summary of Standards |
Group Members |
|
HIC 1 |
The organization has comprehensive and coordinated Hospital
Infection Prevention and Control (HIC) programme aimed at
reducing/eliminating risks to patients, visitors and providers of
care and community. |
1.
Dr. R. Jayaprada, Associate Professor, Dept. of Microbiology
2.
Dr. V. Chandra Sekhar, Asst. Professor, Dept. of Community Medicine
3.
Mrs. M. Lakshmidevi, HICN
4.
Mrs. A. Shoba Rani, HICN
5.
Mrs.K. Karpugam, HICN
6.
Mrs. A. Reddamma, HICN |
|
HIC 2 |
The organization provides adequate and appropriate resources for
infection prevention and control |
1.
Dr. K.V. KotiReddy, RMO
2.
Dr. G. SwethaRao, Asst. Professor, Dept. of Psychiatry
3.
Mrs.E. Bhuvaneswari, NS Gr-II
4.
Mrs.S. Shakira, Head Nurse |
|
HIC 3 |
The organisation implements the infection prevent in and control
programme in clinical areas. |
1.
Dr. K. M. Bhargav, Asst. Professor, Dept. of Medicine
2.
Dr.M. Bhagya Lakshmi, Asst. Professor, College of Nursing
3.
Mrs.G. Indiramma, NS Gr-II
4.
Mrs. J. Saradadevi, NS Gr-II
5.
Mrs. I. Kanthamma, NS Gr-II |
|
HIC 4 |
The organisation implements the infection prevention and control
programme in support services. |
1.
Dr. S. Yamini, Asst. Professor, Dept. of Microbiology
2.
Mr. TVP. Kumar, AE (Tech.)
3.
Mrs. T. Prabhavathi, AD Nursing
4.
Mrs. M. Sunitha Devi, Chief Dietician
5.
Mrs. A. Umamaheswari, Sanitary Dept.
6.
Mr. M. KanthaRao, Sanitary Supervisor |
|
HIC 5 |
The organisation takes actions to prevent healthcare associated
infection (HAI) in patients. |
1.
Dr. A.V. ChaitanyaBhanu, Jr.Resident, Dept. of Dentistry.
2.
Dr. S. Noble Ujeesh, Sr. Resident, Dept. of Microbiology
3.
Mrs.Y. Nirmala, Head nurse (RICU)
4.
Mrs.T. Suseela, Head Nurse ( MICU)
5.
Mrs.K. Rajitha, Staff Nurse, (NABH cell)
|
|
HIC 6 |
The organisation performs surveillance to capture and monitor
infection prevention and control data. |
1.
Dr. N. Ramakrsihna, Asst. Professor, Dept. of Microbiology
2.
Mrs.V. Radha Rani, Head Nurse
3.
Mrs. D. Mary Susella , Head Nurse
4.
Mrs. A. Shoba Rani, Head Nurse |
|
HIC 7 |
Infection prevention measures include sterilization and /or
disinfection of instruments, equipment and devices. |
1.
Dr. R. Jayaprada, Associate Professor, Dept. of Microbiology
2.
Mrs. T. Prabhavathi, AD Nursing
3.
Mrs.B. Prameela, Staff Nurse, (CSSD)
4.
Mr.T.Gangadhara, Sr. Autoclave Tech. |
|
HIC 8 |
The organisation takes action to prevent or reduce healthcare
associated infection in its staff. |
1.
Dr. V. Sameeraja, Asst. Professor, Dept. of Medicine
2.
Dr. G. VisweswaraRao,Asst. Professor, Dept. of Community Medicine
3.
Mrs.J.M. Malathi, Head Nurse
4.
Mrs. C. Reddy Vasantha, Head Nurse |
Chapter 6 : Patient Safety and Quality Improvement
Group Leader :
Dr
V S Kiranmayi, Dept. of Biochemistry
Co-ordinator :
Dr
R. Arun, Dept. of Transfusion Medicine
|
Task code
(Standard) |
Summary of Standards |
Group Members |
|
PSQ 1 |
The organization implements a structured patient-safety programme. |
1.
Dr.Pallavi Chalivendra, Asst. Prof., Dept. of Pharmacology.
2.
Mr P.P. Reddy, Driver, PRO office
|
|
PSQ 2 |
The organization implements a structured quality improvement and
continuous monitoring programme. |
1.
Dr B. Deepthi, Asst. Prof., Dept. of Pathology.
2.
Mrs.V. Radha Rani, Head Nurse
|
|
PSQ 3 |
The organization identifies key indicators to monitor the structures
process and outcomes, which are used as tools for continual
improvement activities. |
1.
Dr B. Hari Prasad, Assoc. Prof., Dept. of General Surgery
2.
Dr N. Lakshmanna, Asst. Prof., Dept. of Biochemistry
3.
Mrs. B. Kokilamma, Asst. Prof., CON |
|
PSQ 4 |
The organization uses appropriate quality improvement tools for its
quality improvement activities. |
1.
Dr D. Ravisankar, Assoc. Prof., Dept. of Community Medicine
2.
Mr P. Ravi, Lab Technician, Dept. of Endocrinology |
|
PSQ 5 |
There is an established system for clinical audit. |
Dr R. Arun, Assoc. Prof., Dept. of Transfusion Medicine |
|
PSQ 6 |
The patient safety and quality improvement programme are supported
by the management. |
1.
Dr A. Surekha, Assoc. Prof., Dept. of Dermatology.
2.
Mr G. Srinivas, Sr. Assist., Accounts Dept. |
|
PSQ 7 |
Incidents are collected and analyzed to ensure continual quality
improvement. |
1.
Dr.Pranabandu Das, Assoc. Professor, Dept. of Radiation Oncology.
2.
Mrs C. Suneetha, Nursing Suptd., Grade-I |
Chapter : 7 - Responsibilities of Management (ROM)
Group Leader :Dr.K.V.Sreedhar Babu,
Professor & Head of Transfusion Medicine
Co-ordinator :
Dr. M. Yerramma Reddy, Dy. Registrar
|
Task code
(Standard) |
Summary of Standards |
Group Members |
|
ROM 1 |
The organization identifies those responsible for governance and
their roles are defined. |
1.
Dr.K.V.SreedharBabu, Professor &
Head of Transfusion Medicine,
2.
Dr. M. Yerramma Reddy, Dy.
Registrar, Purchase |
|
ROM 2 |
The organization is ethically managed by the leaders. |
1.
Dr.D.S. MadhuBabu, Professor
Head, Dept. of Dentistry
2.
Mrs. C. Ushakiran, Assistant
Professor, College of Nursing
|
|
ROM 3 |
The organization is headed by a leader who shall be responsible for
operating the organization on a day-to-day basis. |
1.
Dr. V. Chandra Sekhar, Assistant
Professor, Department of Community
Medicine
2.
Mr. D. Anandbabu, AD,
O/o The Director cum VC
3.
Mrs. P. Nagaprasuna, Superintendent,
Establishment Section
|
|
ROM 4 |
The organization displays professionalism in its functioning |
1.
Dr. D. Srivani,Assistant Professor,
Department of Anatomy
2.
Mrs. G.P. Majula, AD, Establishment
Section
|
|
ROM 5 |
Management ensures that patient-safety aspects and risk-management
issues are an integral part of patient care and hospital management. |
1.
Dr.VinodBhan, Professor,
Department of CT Surgery
2.
Mr. A. NagendraBabu, Supdt.,GM
Office
3.
Mr. Mohan, PA, GM Office
4.
Mr.K. Narasimha Reddy, AE
(Electrical)
|
Chapter : 8 - Facilities Management and Safety (FMS)
Group Leader
: Dr. R. Ram, Medical Superintendent
Co-ordinator
:
Mrs. M. Prasana Lakshmi, Dy. Director (GM)
Mr. E. Doraiswamy, Sr. BME
|
Task code
(Standard) |
Summary of Standards |
Group Members |
|
FMS 1 |
The organization has a system in place to provide a safe and secure. |
1.
Dr. K. Madhavi, Professor, college of
Physiotherapy,
2.
Mr.ElangoDamodaran,Fire Safety
Officer,
3.
Mr.P.S. PrakashBabu,AE Civil SVIMS
4.
Mr. K. Bannerjee, Sr. Fitter |
|
FMS 2 |
The organization’s environment and facilities operate in a planned
manner and promotes environment friendly measures. |
1.
Mrs. M. Prasana Lakshmi, Dy. Director (GM),
2.
P.S. PrakashBabu,AE Civil SVIMS
3.
Mr. K. Narasimha Reddy, AE (Electrical) |
|
FMS 3 |
The organization environment and facilities operate to ensure the
safety of patients, their families, staff and visitors. |
1.
P.S. PrakashBabu,AE Civil SVIMS
2.
Mr. B. Prakash, Security Officer
3.
Mr. K. Narasimha Reddy, AE Electrical
4.
Mrs. C. Sunitha, Nursing Supt. Gr-I ,
5.
4.Dr. EGTV Kumar, Sr. Tech. |
|
FMS 4 |
The organization has a programme for the facility, engineering
support services and utility system. |
1.
Mrs. M. Prasana Lakshmi, Dy. Director (GM),
2.
Mrs. T. Prabhavathi, AD Nursing,
3.
Mr. S. Maheshwarnath, AC Plant Tech.
4.
Mr. K. Narasimha Reddy, AE Electrical
5.
Mrs. C. Sunitha, Nursing Supt. Gr-I, .
6.
Mr. K. Bannerjee,Sr. Fitter,
7.
Mrs. B. Prameela, Staff Nurse, CSSD, |
|
FMS 5 |
The organization has a programme for medical equipment management. |
Mr. E. Doraiswamy, Sr. BME |
|
FMS 6 |
The organization programme for medical gases, vacuum and compressed
air. |
Mrs. M. Prasana Lakshmi, Dy. Director (GM) and Gas Room Operating
Staff Members |
|
FMS 7 |
The organization has a plan for fire and non-fire emergencies within
the facilities. |
1.
Mr.Elango Damodaran, Fire Safety
Officer & Fire Safety Team,
2.
Mr. K. Narasimha Reddy, AE Electrical
3.
Mr. B. Prakash,Security Officer
4.
Mr. K. KanthaRao, Sanitary Supervisor
5.
Mr. NVS. Prasad,MSW
6.
Mrs. M. Prasana Lakshmi, Dy. Director
7.
(GM) and Staff Members
8.
Mr. TVP. Kumar, AE Water Workers
9.
Mrs. T. Prabhavathi, AD Nursing |
Chapter: 9 Human Resource Management (HRM)
Group Leader: Mr. G. Suresh Kumar, A.D-I (Estt.
Sec.)
Co-ordinator:
Smt. G. P. Manjula,
A.D -II (Estt.Sec.)
|
Task code
(Standard) |
Summary of Standards |
Group Members |
|
HRM 1 |
The organization has a documented system of human resource planning. |
1. Dr. K. V. SreedharBabu, Registrar
2. Mr.G. Suresh Kumar, A.D-I (Estt. Sec.)
3. Mrs.G.P. Manjula, A.D-II (Estt. Sec.)
4. Mrs.P. Naga Prasuna, Supdt.,
5. Mrs.V. Aruna, Supdt.,
6. Mr.M. VenkataRamana Reddy, Supdt., |
|
HRM 2 |
The organization implements a defined process for staff recruitment. |
1. Mrs.P. Naga Prasuna, Supdt.,
2. Mrs.V. Aruna,Supdt.,
3. Mr.M. VenkataRamana Reddy, Supdt., |
|
HRM 3 |
Staff are provided induction training at the time of joining the
organization. |
1. Mrs.P. Naga Prasuna, Supdt.,
2. Mrs.V. Aruna, Supdt., |
|
HRM 4 |
There is on-going programme for professional training and
development of the staff. |
1. Mrs.P. Naga Prasuna, Supdt.,
2. Mrs.V. Aruna, Supdt.,
3. Mr.G. Babu, A.D. |
|
HRM 5 |
Staff are appropriately trained based on their specific job
description |
1. Mrs. P. Nagaprasuna, Superintendent,
Establishment Section
2. Mrs C. Suneetha, Nursing Suptd.,
Grade-I
|
|
HRM 6 |
Staff are trained in safety and quality-related aspects. |
1. Dr. R. Jayaprada, Assoc.Professor,
Dept. of Mircrobiology
2. Dr. V S Kirnamayi, Assoc. Professor,
Dept. of Biochemistry
3. Mr.ElangoDamodaran Reddy Fire
Safety Officer
4. Mr. B. Prakash,Security Officer
|
|
HRM 7 |
An appraisal system for evaluating the performance of staff exits as
an integral part of the human resource management process. |
1. Mr. G. Suresh Kumar, A.D-I (Estt. Sec.)
2. Mrs. G. P. Manjula , A.D -II (Estt.Sec.)
3. Mrs. M. Prasana Lakshmi, DD (GM)
4. Mrs. T. Prabhavathi, AD Nursing |
|
HRM 8 |
Process for disciplinary and grievance handling is defined and
implemented in the organization. |
1. G. Suresh Kumar,A.D-I (Estt. Sec.)
2. G. P. Manjula, A.D-II (Estt. Sec.) |
|
HRM 9 |
The organization promotes staff well-being addresses their health
and safety needs. |
1. Dr. V. Vanajakshamma, Professor, Cardiology & Team
2. Mr. M. VenkataRamana Reddy, Supdt.,
3. Mr. A. Rama SubbaRamudu, Supdt.,
4. Mr.K.Giri Babu, AMRO |
|
HRM 10 |
There is a documented personal information for each staff member. |
1. P. Naga Prasuna, Supdt.,(Estt. Sec.)
2. A. Rama SubbaRamudu, Supdt.,
(Estt. Sec.)
|
|
HRM 11 |
There is a process for credentialing and privileging of medical
professionals, permitted to provide patient care without
supervision. |
1. Dr.AlokSachan, Prof & HOD,
Dept. of Endocrinology
2. Dr. B. Manilal, Assoc. Prof, Surgical
Oncology
3. Dr. K. Venkat, Assoc. Prof, Neuro
Surgery
4. Mr. G. Suresh Kumar,A.D -I (Estt. Sec.)
5.Mrs. P. Naga Prasuna, Supdt.,
|
|
HRM 12 |
There is a process for credentialing and privileging of nursing
professionals, permitted to provide patient care without
supervision. |
1. Dr. BCM. Prasad, Professor, Dept. of
Neurosurgery
2. Ms. T. Prabhavathi, A.D (Nursing)
3. Dr. P. Sudharani, Professor, College of
Nursing
4. Mrs.G.P. Manjula,A.D -II(Estt. Sec.)
5. Mrs.V. Aruna, Supdt., (Estt. Sec.)
|
|
HRM 13 |
There is a process for credentialing and privileging of
para-clincial professionals, permitted to provide patient care
without supervision. |
1. Dr. B. VenkataRamana,Assoc.Prof,
Microbiology
2. G. Suresh Kumar,A.D-I (Estt. Sec.)
3. M. VenkataRamana Reddy, Supdt.,
|
Chapter: 10 Information Management System (IMS)
Group Leader :
Mrs. K. Bhavana, IT Manager
Co-ordinator :
Mr. R. Sandeep Kumar, AMRO
|
Task code
(Standard) |
Summary of Standards |
Group Members |
|
IMS 1 |
Information needs of the patients, visitors, staff, management and
external agencies are met. |
1. Mrs.K.Bhavana, IT Manager
2. Mrs.I.Kanthamma, Nursing Supdt.,
Grade-II
3. Mr.B.Prasad (Computer Assistant) |
|
IMS 2 |
The organisation has process in place or management and control of
data and information |
1. Mr.Pranayatheja (Network
Admintrator)
2. Mr. A.Savithri H/N, urology |
|
IMS 3 |
The patients cared for by the organization have a complete and
accurate medical record. |
1. Mr.K.GiriBabu, AMRO and
2. Mr. B.Prasad, Computer Assistant. |
|
IMS 4 |
The medical records reflects the continuity of care. |
1. Mr.K.GiriBabu, AMRO
2. Mr.R. Sandeep Kumar, AMRO |
|
IMS 5 |
The organization maintains confidentiality, integrity and security,
data and information. |
1. Dr.K.V. Koti Reddy, RMO,
2. Dr.P. PrabhanjanKumar , Asst. Prof.
Dept. of Ophthalmology
3. Mr. R. Sandeep Kumar, AMRO |
|
IMS 6 |
The organization ensures availability of current and relevant
documents, records, data and information and provides for retention
of the same. |
1. Mr. K.S. Mohan Srinivas, Royal,
Supdt., MRD
2. Mr.R. Sandeep Kumar, AMRO |
|
IMS 7 |
The organization carries out a review of medical records. |
1. Dr. D.T. Katyarmal, Professor,
Dept. of Medicine
2. Mr.N.S.R.Muralikrishna, MRO,
Dr. YSR Arogyasri Dept.
3. Mr. K.S. Mohan Srinivas, Royal,
Supdt., MRD
4. Mrs.C. .Sunitha, Nursing Supdt.,
Grade-I
|
Home
SVIMS Hospital is committed to promote patient centeredness and ensure
patient safety through continuous quality improvement.
The hospital committees are multi-plural and are formed with care
to include the many facets that are needed for an integrative service
approach. The safety of the patient and the health care workers is the
primary objective of the hospital committees.
Constituted
Committees:
|
Sl. No. |
Chapter |
Name of |
|
01. |
COP |
CPR Analysis Committee (CPRA). |
|
02. |
COP |
Blood Bank Committee |
|
03. |
MOM |
Pharmaco Therapeutics Committee (PTC) |
|
04. |
HIC |
Infection Control Committee |
|
05. |
HIC |
AMS Committee |
|
06. |
PSQ |
Patient Safety Committee |
|
07. |
PSQ |
Quality Improvement Committee |
|
08. |
PSQ |
Sentinel Events Analysis Committee |
|
09. |
HRM |
Internal Complaints Committee |
|
10. |
HRM |
Disciplinary & Grievance Committee |
|
11 |
IMS |
Medical Records Review Committee |
1. CPR
ANALYSIS COMMITTEE:
|
S. No. |
Name |
Role |
Responsibility |
-
|
Medical Superintendent |
Chairperson |
Head & approving authority for Code Blue committee related matters.
Supervise the committee functioning. Reconstitute the committee
whenever required. Take actions for resolution of issues/problems
identified by other committee members. Continuous monitoring of the
quality of the committee functions. |
-
|
RMO |
Member |
Head & approving authority for Code Blue committee related matters.
Supervise the committee functioning. Reconstitute the committee
whenever required. Take actions for resolution of issues/problems
identified by other committee members. Continuous monitoring of the
quality of the committee functions. |
-
|
Dr. A.N. Sowmya (EMD Physician) |
Member |
·
Convene the meeting s with prior approval from Chairperson
·
Conduct Mock drills, audits & debriefing sessions.
·
Attend CPRA monthly BLS & ACLS training programmes. Follow the
instructions given and/or responsibilities assigned by the
Chairperson.
·
Identify the deficiencies and problems to be rectified to improve
the quality of the work.
|
-
|
Dr. Sameraja (General Physician) |
Member |
-
|
Dr. Rama
(General Physician)
|
|
-
|
Dr. Vinay
(Anaesthesiology)
|
Member |
-
|
Dr. Rajamani
(General Physician)
|
|
-
|
Dr. Akila
(Obstretics)
|
|
-
|
Dr. Krian
(Cardiology)
|
|
-
|
Dr. Sreedevi
(Anaesthesiology)
|
|
-
|
Smt. S. Sunitha (NS-I)
Smt. J. Sarada Devi (NS-II)
Smt. G. Indiramma (NS-II)
Smt. I. Kanthamma (NS-II)
Smt. E. Bhuvaneswari (NS-II) |
Member |
Attend CPRA monthly meetings. Arrangements for training programs.
Resource arrangements for Code Blue activities. CAPA analysis and
implementation.
|
-
|
Smt. Y. Nirmala
(Head Nurse)
|
Member |
Attend CPRA monthly meetings. Arrangements for training programs.
Resource arrangements for Code Blue activities. CAPA analysis and
implementation. Follow the instructions given and/or
responsibilities assigned by the Chairperson. Identify the
deficiencies and problems to be rectified to improve the quality of
the work. |
-
|
Smt. T. Suseela
(Head Nurse)
|
Member |
-
|
Smt. L. Haritha
(Head Nurse)
|
Member |
-
|
Smt. N. Ravanamma
(Head Nurse)
|
Member |
-
|
B. Divyavani
(Code Blue Nurse)
|
Member Secretary |
·
Attending the Code Blue calls.
·
Maintaining the Code Blue data base. Collection and documentation of
Code Blue census.
·
Follow-up of the Code Blue survivors.
·
Attend CPRA review meetings.
·
Identifying the shortfalls in resources and address them to the
Nursing Superintendent / CPRA committee.
·
Participate in Mock drills and audits. |
-
|
P. Geetha
(Code Blue Nurse)
|
Member |
-
|
G.Ramasri
(Code Blue Nurse)
|
Member |
-
|
P. Chandana
(Code Blue Nurse)
|
Member |
-
|
P. Haritha
(Code Blue Nurse)
|
Member |
-
|
G. Sunil |
Member |
|
-
|
D. Manjusha |
|
|
-
|
G. Praveen Kumar |
|
|
-
|
Mr. B. Prasad (IT Department) |
Member |
Coordinate the members of the committee. Making arrangement for the
meetings. Documentation minutes of the meetings. Records
maintenance. Follow the instructions given and /or responsibilities
assigned by the Chairperson. |
-
|
Mr. N.VS. Prasad |
MSW |
Counselling the patient attendants during Code Blue. Follow the
instructions given and/or responsibilities assigned by the
Chairperson. |
-
|
Mr. Prakash |
Security |
Attend all Code Blue calls & provide support for the Code Blue Team.
Assist with way finding for staff, and other patients/visitors.
Cordon off the area to ensure the Code Blue Team is unimpeded.
Controlling the attendants during Code Blue. Follow the instructions
given and/or responsibilities assigned by the Chairperson. |
Meeting schedule and quorum of the meeting
·
CPRA committee review meetings are being conducted once in a month
preferable on second Monday of every month.
·
Quorum:
requires at least 50% of the total committee members i.e., minimum of 10
members.
·
Presence of Cardiologist/General Physician, Anaesthesiologist, Nursing
Superintendent, Head Nurse, Nurse from Code Blue team, MSW, Security
officer during the review meetings is mandatory to fulfil the quorum.
Home
2.
INFECTION CONTROL COMMITTEE:
HOSPITAL
INFECTION CONTROL COMMITTEE MEMBERS
|
S. No |
Name |
Role |
Responsibility |
|
1 |
Director cum Vice-Chancellor |
Chairman |
Head & approving authority for committee related matters. Supervise
the committee functioning. |
|
2 |
Dr Ram |
Co-chairman |
Reconstitute the committee whenever required. Take actions for
resolution of issues/problems identified by other committee members.
Continuous monitoring of the quality of the committee functions. |
|
3 |
Dr B. Venkata Ramana |
Member secretary |
Senior Microbiologist. Monitors the activities of Infection control
team. |
|
4 |
Dr A. Mohan |
Member |
Take actions for resolution of issues/problems identified by other
committee members. Continuous monitoring of the quality of the
committee functions. |
|
5 |
Dr Pranabandhu Das |
Member |
Take actions for resolution of issues/problems identified by other
committee members.
Attend monthly review meetings. Follow the instructions given and/or
responsibilities assigned by the Chairperson/Co-chairperson |
|
6 |
Dr G. Swetha Rao |
Member |
Take actions for resolution of issues/problems identified by other
committee members.
Attend monthly review meetings. Follow the instructions given and/or
responsibilities assigned by the Chairperson/Co-chairperson |
|
7 |
Dr Chaitanya |
Member |
Take actions for resolution of issues/problems identified by other
committee members.
Attend monthly review meetings. Follow the instructions given and/or
responsibilities assigned by the Chairperson/Co-chairperson |
|
8 |
Dr C. Konda Reddy |
Member |
Take actions for resolution of issues/problems identified by other
committee members.
Attend monthly review meetings. Follow the instructions given and/or
responsibilities assigned by the Chairperson/Co-chairperson |
|
9 |
Dr D. Satyavathi |
Member |
Take actions for resolution of issues/problems identified by other
committee members.
Attend monthly review meetings. Follow the instructions given and/or
responsibilities assigned by the Chairperson/Co-chairperson
|
|
10 |
Dr Prajakta |
Member |
Take actions for resolution of issues/problems identified by other
committee members.
Attend monthly review meetings. Follow the instructions given and/or
responsibilities assigned by the Chairperson/Co-chairperson |
|
11 |
Dr R. Jayaprada |
HICO |
Coordinate with the Medical Superintendent (Co-Chairman) in planning
infection control program and measures.
ICO is responsible for surveillance and supervision of hospital
acquired infection as well as preventive and corrective programmes
in the hospital. |
|
12 |
Dr N. Ramakrishna |
HICO |
|
13 |
Dr S. Yamini |
HICO |
|
14 |
Dr V. Harika |
HICO |
|
15 |
Mrs. T. Prabhavathi |
Member |
Attend monthly review meetings.
Follow the instructions given and/or responsibilities assigned by
the Chairperson / Co-chairperson |
|
16 |
Mrs. M. Lakshmidevi |
Member |
Environmental surveillance.
Surveillance of air in OT’s/ICUs.
To check for sterilization & dis-infection practices.
In-use test of disinfectants.
Autoclave checks.
Water testing.
Continuous surveillance of HAI infections.
Educating of HCWs. |
|
17 |
Mrs. V. Karpugam |
Member |
|
18 |
Mrs. D. Redemma |
Member |
|
19 |
Mrs. A. Shobharani |
Member |
|
20 |
Mrs. Shakira |
Member |
Monitor OT related IPC practices, Attend monthly review meetings.
Follow the instructions given and/or responsibilities assigned by
the Chairperson / Co-chairperson. |
|
21 |
Mrs. C. Sunitha |
Member |
Monitor CSSD related IPC practices, Attend monthly review meetings.
Follow the instructions given and/or responsibilities assigned by
the Chairperson/Co-chairperson. |
|
22 |
Mrs. A. Umamaheswari |
Member |
Monitor sanitation & disinfection activities in all areas, Attend
monthly review meetings.
Follow the instructions given and/or responsibilities assigned by
the Chairperson/Co-chairperson. |
|
23 |
Dr P. Subramanyam |
Member |
Monitor Antimicrobial prescriptions for high end antibiotics and
antimicrobial prescription audit.
Attend monthly review meetings.
Follow the instructions given and/or responsibilities assigned by
the Chairperson/Co-chairperson. |
|
24 |
Mrs.C. Sunitha |
Member |
Monitor Laundry & linen related IPC practices, Attend monthly review
meetings.
Follow the instructions given and/or responsibilities assigned by
the Chairperson/Co-chairperson. |
|
25 |
Mrs. D. Indiramma |
Member |
|
26 |
Mrs.M. Sunitha |
Member |
Monitor Kitchen sanitation & vaccination of food handlers. Attend
monthly review meetings.
Follow the instructions given and/or responsibilities assigned by
the Chairperson/Co-chairperson. |
|
27 |
Dr V. Chandrasekar |
Member |
Monitor any outbreaks if infections & MDR bugs.
Attend monthly review meetings.
Follow the instructions given and/or responsibilities assigned by
the Chairperson/Co-chairperson. |
|
28 |
Mr. T.V.P.Kumar |
Member |
Monitor water tanks disinfection including RO plants.
Attend monthly review meetings.
Follow the instructions given and/or 28responsibilities assigned by
the Chairperson/Co-chairperson. |
|
29 |
Mr. P. Yashodhar |
Member |
Air and surface surveillance culture for OT, ICU’s and other high
risk areas
Performing water surveillance to test the quality for drinking water
Performing disinfectant testing of a range disinfectant
Sterility checking of blood and blood product |
|
30 |
Mr. V. Venkatesh |
Member |
|
31 |
Mr. Sai Jagadeesh |
Secretarial
Assistant
|
Documentation of minutes of the meetings. |
Meeting schedule and quorum of the meeting
·
HICC committee
review meetings are being conducted once in a month preferably on
FIRST TUESDAY of every month.
·
Quorum:
Requires at least 50% of the total committee members i.e., minimum of 15
members.
·
Presence of
Chairperson/Co-chairperson, member secretary, Physicians, surgeons,
HICOs, ICNs, Nursing superintendent, health inspector, CSSD, engineering
dept., OT and ICUs in charges during the review meetings is mandatory to
fulfil the quorum.
3.
PHARMACO THERAPEUTICS COMMITTEE:
|
S.No |
Name |
Role |
Responsibility |
|
1 |
Dr.Ram
(Medical Superintendent) |
Chairman |
Advising medical, administrative and pharmacy departments on
pharmaceutical related issues.
Monitor and Supervise the committee functioning. Reconstitute the
committee whenever required.
|
|
2 |
Dr.K.Uma Maheswara Rao
(Prof & HOD, Pharmacology) |
Executive Secretary |
Developing drug policies and procedures.
Evaluating and selecting medicines for the formulary and providing
for its periodic revision. Promoting & conducting effective
interventions to improve medication use. Monitoring ADRs &
Medication errors. Conducting audits and training programmes for
improving medication safety.
|
|
3 |
Dr.P.Subramanyam
(Sr.Pharmacist) |
Member |
Attend PTC monthly meetings. Following the instructions assigned by
the chair person and executive secretary. Checking whether
medications are stored appropriately and are available when
required. Checking whether medications are dispensed in safe manner.
Checking whether medical supplies and consumables are stored
appropriately and are available when required. Identifying
deficiencies to improve the quality of medication safety.
|
|
4 |
Dr. Aloka Samantaray
(Prof & HOD, Anaesthesiology)
|
Member |
Attend PTC monthly meetings. Reviewing the minutes of meetings.
Checking for the proper maintenance of crash cart.
|
|
5 |
Dr.Vinod Bhan
(Prof., CT Surgery)
|
Member |
Attend PTC monthly meetings. Reviewing the minutes of meetings.
Checking whether implantable prosthesis and medical devices are used
in accordance with laid down criteria.
|
|
6 |
Dr.Chandramalitheswaran
(Assoc. Prof, Surgical GE)
|
Member |
Attend PTC monthly meetings. Reviewing the minutes of meetings.
Advising for surgical items and their storage.
|
|
7 |
Dr.Malathi
(Assoc.Prof, OBG)
|
Member |
Attend PTC monthly meetings. Reviewing the minutes of meetings. |
|
8 |
Dr.Venkata Naveen Prasad
(Assoc Prof, Neurology)
|
Member |
Attend PTC monthly meetings. Reviewing the minutes of meetings.
|
|
9 |
Dr.Bhargavi
(Assoc Prof., Medical Oncology)
|
Member
|
Attend PTC monthly meetings. Reviewing the minutes of meetings.
Checking whether narcotic drugs and psychotropic substances,
chemotherapeutic agents are used safely. |
|
10 |
Dr.M.C.R.Rama
(Asst.Prof.,of Medicine)
|
Member |
Attend PTC monthly meetings. Reviewing the minutes of meetings. |
|
11 |
Dr.Harini Devi
(Assoc.Prof.,Biochemistry)
|
Member |
Attend PTC monthly meetings. Reviewing the minutes of meetings.
Advising regarding lab chemicals, reagents and their storage
|
|
12 |
Dr.Sujith Kumar
(Assoc. Prof, Community Medicine)
|
Member |
Attend PTC monthly meetings. Reviewing the minutes of meetings. |
|
13 |
Dr.Akhila
(Asst.Prof.,OBG)
|
Member |
Attend PTC monthly meetings. Reviewing the minutes of meetings. |
|
14 |
Dr.C.Pallavi
(Asst.Prof., Pharmacology) |
Member |
Attend PTC monthly meetings. Attending clinical audits and training
programmes related to medication safety. Monitoring medication
errors and CAPA. Reviewing the minutes of meetings.
|
|
15 |
Dr.G.Ravindra Kumar
(Asst.Prof., Pharmacology) |
Member |
Attend PTC monthly meetings. Attending clinical audits and training
programmes related to medication safety. Monitoring medication
errors and CAPA. Reviewing the minutes of meetings. |
|
16 |
Dr.Ramya Priya
(Asst.Prof., Nuclear Medicine)
|
Member |
Attend PTC monthly meetings. Reviewing the minutes of meetings. |
|
17 |
Dr.Jayaprda
(Assoc.Prof. Microbiology)
|
Member |
Attend PTC monthly meetings. Reviewing the minutes of meetings.
Monitoring Antibiotic audit Committee and developing policies
concerning usage of antibiotics.
|
|
18 |
Dr.M.Yerram Reddy
(A.D Purchase) |
Member |
Attend PTC monthly meetings. Reviewing the minutes of meetings.
Monitoring for improved medicine procurement and inventory
management.
|
|
19 |
Mr.L.Sateesh
(A.D Stores) |
Member |
Attend PTC monthly meetings. Following the instructions assigned by
the chair person and executive secretary. Checking whether
medications are stored appropriately and are available when
required. Checking whether medications are dispensed in safe manner.
Checking whether medical supplies and consumables are stored
appropriately and are available when required. Identifying
deficiencies to improve the quality of medication safety. |
|
20 |
Mrs.Prabhavathi
(A.D. Nursing) |
Member |
Attend PTC monthly meetings. Reviewing the minutes of meetings.
Checking for the safe dispensing and administration of medications.
Monitoring the patients after administration. Advising medication
administration staff to minimise medication errors and take
necessary CAPA for enhancing patient safety. |
|
21 |
Mrs.C.Sunitha
(Nursing Superintendent Gr-I) |
Member |
Attend PTC monthly meetings. Reviewing the minutes of meetings.
Checking for the safe dispensing and administration of medications.
Advising medication administration staff to minimise medication
errors and take necessary CAPA for enhancing patient safety. |
|
22 |
Mr.Subramanyam Raju
(Pharmacist Gr-I) |
Member |
Attend PTC monthly meetings. Reviewing the minutes of meetings.
Checking for the safe dispensing of medicines. |
|
23 |
Mr.Babu Suresh
(Pharmacist Gr-I)
|
Member |
Attend PTC monthly meetings. Reviewing the minutes of meetings.
Checking for the safe dispensing of medicines. |
|
24 |
Dr.A.Sai Kiran
(Clinical Pharmacist) |
Member |
Attend PTC monthly meetings. Reviewing the minutes of meetings.
Attending clinical rounds and monitoring medication use. Identifying
and reporting ADRs medication errors along with CAPA. |
|
25 |
Dr.P.Anuhya
(Clinical Pharmacist) |
Member |
Attend PTC monthly meetings. Reviewing the minutes of meetings.
Checking whether medication orders are written in uniform manner or
not. Attending clinical rounds and monitoring medication use.
Identifying and reporting ADRs medication errors along with CAPA. |
Meeting schedule and quorum of the meeting
·
PTC meeting is scheduled once in a month i.e. every
1st Friday
of month
·
Quorum:
Requires at least 50% of the total committee members
Home
4.
QUALITY IMPROVEMENT COMMITTEE:
|
Sl. No. |
Name & Designation of the Member |
Position in the committee |
Roles and Responsibilities of the member |
|
01 |
Director cum Vice-Chancellor |
Chairman |
|
|
02 |
Dr. Y. Mutheeswaraiah,
Professor & Head, Dept. of Surgery |
Member |
Implementation of AAC standards through out the hospital. |
|
03 |
Dr. K. UmamaheswarRao,
Professor & Head, Dept. of Pharmacology |
Member |
Implementation of MOM chapter through out the hospital and PSQ3
standard. |
|
04 |
Mrs. K. Bhavana
IT Manager |
Member |
Implementation of IMS chapter through out the hospital |
|
05 |
Mrs. GP. Manjula
AD Establishment Section II |
Member |
Implementation of HRM chapter |
|
06 |
Dr. VinodBhan
Professor, Dept. of C.T. Surgery |
Member – Patient Safety |
Implementation of Patient safety programmes through out the
hospital and PSQ 1, & FMS 3 (e) ( f) |
|
07 |
1.
Dr. A. Surekha, Assoc. Prof., Dept. of DVL – I/c for Medical
Departments
2.
Dr. B. Manilal, Assoc. Prof., Dept. of SO – I/c for Surgical
Departments
3.
Dr. V. Sivakumar, Asst. Prof, Dept. of Pathology – I/c for Lab
Departments |
Member – Clinical safety |
Implementation Clinical Safety measures through out the hospital &
PSQ 4 standard. |
|
08 |
Dr. Pranabandu Das,
Assoc. Professor, Dept. of Radiotherapy
|
Member |
In charge for Sentinel events Analysis & Implementation of PSQ 7
standard |
|
09 |
Dr.H.Narendra Prof. & Head, Dept. of SO |
Member |
In charge for clinical audits and Implementation of PSQ 5 standard |
|
10 |
Dr. R. Jayaprada,
Assoc. Professor, Dept. of Microbiology
|
Member from HIC |
Implementation of HIC programme through out the hospital and
Implementation of PSQ3, FMS 1 (e), FMS 7 (c), standard elements. |
|
11 |
Mr. Elango Reddy,
Fire Safety Officer
|
Member from support services |
Implementation of FIRE SAFETY, Mock drills for CODE RED &
FMS 4 (e) & FMS 7 standard elements.
|
|
12 |
Mr. B. Prakesh,
Security Officer
|
Member from Support services |
FMS 3 (b) |
13 |
Dr V.S.Kiranmayi,
Assoc. Professor, Dept. of Biochemistry
|
Member from Lab services |
Implementation of PSQ, chapter through out the hospital and PSQ 3
standard in detail. |
|
14 |
Dr. V. Vanajakshama,
Professor, Dept. of Cardiology
|
Member from CPR committee |
Implementation of mock drills for code blue FMS 7 (c) |
|
15 |
Dr. J. Malathi,
Assoc. Professor, Dept. of OBG
|
Member from OBG services |
Implementation of mock drills for CODE PINK
, FMS 7 (c) & COP 10 standard elements. |
|
16 |
Dr. Punith Patak,
Assoc. Professor & Ho Di/c, Dept. of Paediatrics
|
Member from Paediatric services |
Implementation of mock drills for CODE PINK, FMS 7 (c) & COP 11
Standard elements.
|
|
17 |
Dr. P. JanakiSubhadhra,
Professor, Dept. of Anaesthesiology
|
Member from ICU services |
Implementation of PSQ3 standard through out the hospital. |
|
18 |
Dr. S. Sarala,
Professor, Dept. of Radiology
|
Member from Imaging Services |
Implementation of RADIATION SAFETY PRACTICES ACROSS IMAGING SERVICES
- AAC 9, AAC10, & AAC 11 standards. |
|
19 |
HoD EMD Services |
Member from Emergency Services |
Implementation of PSQ3, COP 2, COP3, COP 4 & FMS 7 (c) standards
and elements |
|
20 |
Mr. K. Kantha Rao,
Sanitary Supervisor
|
Member – Support Services |
Implementation of HIC 4(c) through out the hospital.
|
|
21 |
Mrs. M. Prasanna Lakshmi,
Deputy Director (GM)
|
Member – Facility Management |
Implementation of FMS 2 (g), FMS 3 (e), FMS 6 standards and elements
through out the hospital. |
|
22 |
Asst. Engneer, Civil, TTD SVIMS
|
Member – Facility Management |
Implementation of FMS 1 (a, b, e) FMS 2 (b, g) FMS 3 (a) FMS 4 (f)
standards and elements through out the hospital. |
|
23 |
Mr. K. Narasimha Reddy,
Asst. Engineer (Electrical)
|
Member – Facility Management |
Implementation of FMS 2 (b) (d), (e), ( g) FMS 3 (c), FMS 4 (a,),
(b), (c), (d), (e), (f), (g), (h) standards and elements through out
the hospital. |
|
24 |
Mr. T.V.P. Kumar,
Asst. Engineer, Technical
|
Member – Facility Management |
Implementation of FMS 1 b, FMS 2(d, e, f, g)& FMS 4 (c, f, g, h) |
|
25 |
Mr. Dorai Swamy,
Sr. Biomedical Engineer
|
Member from Facility Management |
Implementation of FMS 5 |
|
26 |
Account Officer |
Member from Finance/Accounts |
PSQ6(e) & ROM 4 (c) |
|
27 |
Mr NVS. Prasad
Medico social Worker |
Member from Patient Reported Outcome Measures (PROM) |
PSQ 3 (e) & FMS 7 (c) |
|
28 |
Patient Safety Committee
Leader |
|
Implementation of PSQ1 (a,b,c,d,e,f,g,g,i) FMS 1 (b, d) |
|
29 |
Mr. R. Nagaraja,
Sr. Artist
|
Member |
Implementation of FMS 2 (c) |
|
30 |
Mrs. T. Prabhavathi
Asst. Director (Nursing) |
Member from Nursing Services |
Implementation of FMS 3 (e), FMS 4 (d) |
Meeting schedule and quorum of the meeting
·
The quality improvement meeting is scheduled twice in a month i.e. on
2nd & 4th Tuesday
of every month.
·
The meetings are held by involving limited departments to discuss and
review the quality improvement activities in patients oriented areas and
in the organization oriented standards.
5.
PATIENT SAFETY COMMITTEE:
|
S. No |
Name |
Role |
Responsibility |
|
1 |
Facility Management Team
|
1.1
Principal, College of Physiotherapy |
Provision of Grab Bars, Special Toilets for differently able
persons, wheel chairs, External and Internal signage’s and bed
rails. |
|
|
|
1.2
Deputy Executive Engineer, Civil |
Before commencement of expansion or maintenance of any work, risk
assessment shall be done with the help of HIC coordinator and this
shall be covered noise, vibration and infection control. Built and
updated drawings are to be maintained as per statutory requirements,
Check the swing doors unsafe for people passing through it.
Leakages/seepages in the area rendering it prone to infection.
Height of the ceiling can cause injury to head to people with long
height. Unwanted or unnoticed holes, breaks in the floor/ground
that can be hazardous while walking. Terrace/higher floors lack of
grills at the border making it unsafe. |
|
|
|
1.3
Radiation Safety Officer |
To follow AERB guidelines.
|
|
|
|
1.4 AE,
SVIMS |
Potable water testing, overhead storage cause accidents, Is
placement of furniture can cause any fall. |
|
|
|
1.5
Assistant Engineer, Electrical, TTD |
Electricity Back up, Elevators movements to avoid sudden
stoppage and jerks, unprotected electrical wirings, lack of adequate
lighting can cause which can be reason for accidents or errors.
|
|
|
|
1.6
Security Officer |
Restricted entry into OTs, ICUs and CC TV coverage of the
entire hospital and monitoring. |
|
|
|
1.7
Deputy Director (GM) |
As per FMS 7 standard |
|
|
|
1.8
Deputy Director (GM) |
As per FMS 6 standard |
|
|
2. Dr. Vinod Bhan, Professor, Department of CT Surgery
|
Patient Safety Officer |
1.
Environmental Safety
2.
Lab Safety
3.
Equipment risk Eg. Fire/Injury risk from use of LASER
4.
Risk resulting from long term conditions
5.
Internal and External reporting system on process failure
6.
Fire accidents
7.
Leakage of radiation source
8.
Incidents covering from “no harm” to “sentinel events”
9.
Pro-active risk analysis of patient safety risks shall be done
through HIRA and FMEA.
10. At
minimum one patient safety related risk shall undergo proactive risk
analysis every year.
11.
Avoid Lack of continuity of manpower during surgery due to shift
duties
12.
Avoid Patient Fall from trolley to bed and bed to Trolley
13.
Avoid Cautery burns
14.
Avoid Delay in availability of surgical material in middle of
surgery
15.
Connecting all critical equipments to UPS
16.
Continuous medical gas supply
17.
Patient safety officer shall report directly to the top management
|
|
|
|
Clinical Safety Officer |
1.
Radiation Safety – ALARA (As low as reasonably achievable) Eg. X-ray
for all ICU, Pediatric or neonatal, patients. CT Scan protocols
to be modified to use the lowest exposure. Parameters to maintain
the image quality appropriate for clinical indication. Eg. CT for
ur eteric calculi can be done with low dose where as renal tumor
will require high dose.
2.
Appropriate screening of the patients before imaging.
3.
Patients in the child bearing age group who need to be exposed to
radiation should be scanned for pregnancy. MRI patients screened
for Magnetic substance. Screening also shall be applicable to the
accompanying patient/child into the imaging area.
4.
Shielding of body parts of the patients, attendants shall be adhered
to using appropriately.
5.
To identify various risk, record for action taken for risk
alleviation of each of these risk and the mechanism for informing
the staff regarding the same.
6.
Medication Management covering the issues of Patient/Service user,
allergies and antibiotic resistance.
7.
Implementation of current national patient safety/International
patient safety goals.
8.
SBAR communication for patients handover
9.
Two identifiers for patients identification
10.
Implement evidence based medicine/ clinical practice guidelines (STGs)
Standard Treatment Guidelines bought by GoI.
11. To
define list of high risk medication, Look alike sound alike,
different concentrations of the same drug to be stored far away,
High risk medications are to be verified before dispensing,
Inadvertent administration of drug through wrong route shall be
avoided.
12.
Medication orders shall be checked at transition points of the
patients.
13.
Hand Hygiene guidelines at all locations of hand washing areas.
14. One
Needle, one syringe and only one time policy. To implement CDC
recommendations.
15.
Retained missing instruments and gauze |
|
|
|
Paramedical staff |
1.
Follow HIC practices while attending patients.
2.
Avoid to storing of listed hazardous material in unsafe condition
3.
Maintain MSDS sheets |
|
|
|
Clinicians
|
1.
Implementation National/International patient Safety Goals
2.
Implement the Clinical Safety Officer guidelines pertaining to the
respective Clinical and Diagnostic departments as suggested by the
Clinical Safety Officer.
3.
Implement evidence based medicine/ clinical practice guidelines (STGs)
Standard Treatment Guidelines bought by GoI. |
|
|
|
Nurses |
1.
Implement the guidelines pertaining to the respective clinical
departments as suggested by the Clinical Safety Officer.
2.
Follow HIC practices while attending patients.
3.
Fall risk assessment of the patients and to take pro-active risk
management. |
|
|
|
Support Services |
1.
Slippery floor and probable to cause slip falls.
2.
Rodents and pests in the area which can cause harm to patients,
staff and equipments. |
Meeting schedule and quorum of the meeting
·
The Patient safety committee meeting is scheduled once in a month i.e.
on
4th Saturday
of every month.
·
Quorum:
Requires at least 50% of the total committee members
·
Patient safety aspects like development, implementation and monitoring
of the safety plans and policies to provide as safe and secure facility
and environment. Proactive risk assessment, FEMA, HIRA, facility
inspection rounds, patient safety incident, risk management and analysis
of key-safety indicators and sentinel events.
6.
INTERNAL COMPLAINTS COMMITTEE:
|
S. No. |
Name of the Member |
Designation & Department |
Status in Internal Complaints Committee |
|
01 |
Dr Aparna R Bitla |
Professor, Department of Biochemistry |
Presiding Officer |
|
02 |
Dr.V.Venkatarami Reddy |
Professor & HOD, Department of Surgical G.E. |
Member |
|
03 |
Dr.K.Prathiba |
Associate Professor, Department of Anatomy |
Member |
|
04 |
Sri. Ashok Kumar |
Advocate & Standing Counsel, SVIMS |
Member-External (legal) |
The respective HoD’s /College Principals/Administrative HoD’s shall be
co-opted on case to case basis depending upon the need.
Roles & Responsibilities
The Internal Committee, SVIMS plays an important role in the functioning
of the provisions of the Act and to ensure the fulfillment of its
objectives of the Internal Committee Policy thus the main function of
the Internal Committee is:
·
Implementation of the Internal Committee Policy relating to the
prevention of sexual harassment.
·
Resolving complaints by the aggrieved based on the guidelines of the
Internal Committee Policy.
·
Recommending actions to be taken by the Employer.
As per Section 11(3) the internal Committee enjoys the powers same as
that of a civil court and therefore:
·
It is empowered to initiate an inquiry into a complaint of sexual
harassment at the workplace according to the Internal Committee Policy.
·
IC has the power to summon witnesses and parties to state the committee.
·
It enjoys the discretion of summoning evidence to be examined if it may
be deemed necessary to do so by the members of the committee.
·
All the members thus have an active role in each of the above. The
external legal advisor shall give opinion related to the legal issues
pertaining to the case. Inclusion of the external member ensures
transparency and authenticity to the entire process and gives an outside
perspective.
Responsibilities of Internal Complaints Committee:
SVIMS is bound by Prevention of Sexual Harassment Act and displays the
names and details of the current IC members on the premises at prominent
places as well as in the official website.
·
Receive complaints of sexual harassment at the workplace
·
Initiate and conduct an inquiry as per the policy
·
Submit findings and recommendations of all such inquiries
·
Maintain strict confidentiality throughout the process as per
established guidelines of the Internal Committee Policy
·
Submit annual report in the prescribed format as prescribed.
Meeting schedule and quorum of the meeting
·
Once in a month and as and when a case is registered, the committee
shall meet immediately.
·
Quorum:
Requires 100% of the total committee members.
7.
DISCIPLINARY & GRIEVANCE COMMITTEE:
|
S. No. |
Name of the Member |
Status in Disciplinary & Grievance Committee |
Roles &
Responsibility |
|
01 |
Dr. D. Rajasekhar |
Chairperson |
The Grievance Committee shall be responsible to ensure that
grievances are dealt with effectively in accordance with the
Grievance Procedures set out for the implementation of this
Policy.
In doing so, the Committee shall adhere to the following principle
·
Take grievances seriously taking on board why the employee feels
aggrieved, unhappy or dissatisfied
·
Investigate the facts and surrounding circumstances, and showing
the employees that this been done thoroughly and sensitively.
·
Actively look for a solution that will satisfy the employee, where
practical without causing disproportionate difficulty for the
organization or the Employee’s colleagues.
·
Provide feedback to the employee about what can, and cannot be
done to resolve the grievance
·
Take necessary follow-up action
·
All the members thus have an active role in each of the above.
|
|
02 |
Dr. A. Mohan |
Member – Ex-Officio – Dean
|
|
03 |
Dr. K.V. Sreedhara Babu |
Member – Ex-Officio – Registrar |
|
04 |
Dr. K. Nagaraj |
Member – Secretary |
|
05 |
Dr. Dr. Chandramal Theswaran |
Member |
|
06 |
Dr. K. Prathiba |
Member |
|
07 |
Dr. A. Surekha |
Member |
|
08 |
Dr. M. Ganesh Kumar |
Member |
|
09 |
Dr. V. Srikumari |
Member |
|
10 |
Mrs. G.P. Manjula |
Convener & Coordinator |
Meeting schedule and quorum of the meeting
·
The disciplinary & Grievance Committee meeting shall be held on
1st Saturday
of every month between 3 and 4 pm in the committee hall.
·
Quorum
requires at least 50% of the total committee members.
8.
MEDICAL RECORDS REVIEW COMMITTEE:
|
S.
No. |
Name of the Member |
Status in Disciplinary &
Grievance Committee |
Roles &
Responsibility |
|
01 |
Medical Superintendent |
Chairperson |
·
Responsible or overall supervision of the Committee activities.
·
Responsible for sending lacunas for CAPA to the concerned HoD’s. |
|
02 |
Medical Record Officer |
Coordinator |
·
Co-ordinate the Medical Record Review Committee Meeting.
·
Prepares the minutes of the meeting.
·
Dispatches the minutes to the concerned and inform the deficits to
the concerned.
·
Responsible for sample bases review |
|
03 |
Resident Medical Officer |
Member |
·
Address the members in the meeting, discuss with the concerned
members to complete the lacunas at the earliest. |
|
04 |
HoD, Dept. of Anaesthesiology |
Member |
·
Responsible to conduct audit for complete consent form,
anaesthesia record & operation record. |
|
05 |
HoD, Dept. of Pharmacology |
Member |
·
Responsible to conduct audit for medication chart, regarding
administered drug properly, legibility of author name, signature
time and to write in capitals, using no short forms, dosage. |
|
06 |
Prof. Dept. of Medicine |
Member |
·
To audit the medical cases. |
|
07 |
Assoc. Prof Dept. of General Surgery |
Member |
·
To audit the surgical cases. |
|
08 |
AD Nursing & Nursing Group |
Member |
·
To audit the nursing assessment / Nurses notes and various consent
forms used at the time of admission. |
Meeting schedule of the Medical Record Review Committee meeting
The Medical Record Review committee shall meet once in a month i.e. on
3rd Thursday
at 10:30 am in the committee hall to review the medical records of
current patients.
9.
AMS COMMITTEE
Antimicrobial stewardship is a coordinated program that promotes the
appropriate use of antimicrobials (including antibiotics), improves
patient outcomes, reduces microbial resistance, and decreases the spread
of infections caused by multidrug-resistant organisms.
1. Dr
R. Ram (Medical superintendent)
- Chairman
2. Dr
R. Jayaprada (Microbiology)
- Member
3. Dr
N. Ramakrishna (Microbiology)
- Member
4. Dr
C. Sunil Kumar
(GM)
- Member
5. Dr
M.C.R. Rama (GM)
- Member
6. Dr
C.V.S.Manasa
(GM)
- Member
7. Dr
V. Manolasya,
(GM)
- Member
8. Dr
Surekha.A
(Dermatology)
- Member
9. Dr
B.Hari Prasad
(GS)
- Member
10. Dr V.
Nagateja (Plastic surgery)
- Member
11. Dr
K. Venkat
(Neurosurgery)
- Member
12. Dr
B. Manilal
(SO)
- Member
13. Dr
J. Malathi
(OBG)
- Member
14. Dr
D. Bhargavi
(MO)
- Member
15. Dr
A. Naga Sowmya
(EMD) -
Member
16. Dr
Jonnakuti Rani
(EMD) -
Member
17. Dr
P. Hemalatha
(Anaesthesiology) -
Member
18. Dr C.
Sumadhu (Anaesthesiology)
- Member
19. Dr
V. Chandra sekhar
(PSM) -
Member
20. Dr
K. Vijaya Chandra Reddy
(Pharmacology) - Member
21. Dr
J.P. Joshi Sowmya (Pharm D)
- Member
22. Dr
C. Pallavi
(Pharmacology)
- Member
23. Dr
Peta subramanyam (Pharmacist)
- Member
24. Mr V.
Babu suresh (Pharmacist)
- Member
25. K.V.
Kishore Tangella
- Member
26. AMS &
HIC Link nurses (All ICU and RR) -
Member
27.
Nursing Superintendents (Mrs Indiramma & Mrs Sharada devi) -
Member
Meeting schedule of the Medical Record Review Committee meeting
Ø
The committee shall meet once in a month as per Medical Superintendent
orders.
·
Quorum
requires at least 50% of the total committee members.
Home
|
